
by Jack Norris, Registered Dietitian
Contents
- Summary
- Introduction
- Elevated B12 as a Marker for Disease: Serum B12 and Mortality
- B12 Supplementation Trials
- B12 Observational Studies
- Vitamin B12 and Lung Cancer
- Cyanocobalamin, Cyanide, and Kidney Disease
- Practical Implications
- B12 Supplements and Skin Rashes
- Footnotes
- Bibliography
Note: I used AI for the literature review, data analysis, claim verification, and editing of this article. Last updated: May 2026.
Summary
Elevated vitamin B12 levels in the blood are usually a sign of an underlying health problem, not a cause of one. Liver disease, kidney disease, and various cancers can all raise B12 levels, which is why studies finding associations between high B12 and poor health outcomes are generally measuring the effect of these diseases on B12 levels, not vice-versa.
For vegans who supplement with B12, the evidence is cautiously reassuring. The only large study of healthy adults examining B12 supplement safety found no association between B12 supplementation and increased mortality at any dose, including 1,000 µg/day or more.
There’s one area of genuine uncertainty: Some evidence suggests that very high circulating B12 levels may modestly increase lung cancer risk. The absolute risk is small; roughly 1 in 2,000 people with high B12 levels would develop one additional lung cancer case over six years, and the evidence isn’t conclusive. This isn’t a reason to stop supplementing, but rather to stick to recommended doses rather than taking more than needed. VeganHealth’s recommended supplemental doses result in roughly half of the total B12 absorbed compared to our estimated absorption for the high-risk group in that study.
People with kidney disease should avoid high-dose cyanocobalamin supplements specifically, as there is evidence it may accelerate kidney function decline. Methylcobalamin is a better option for this group.
Supplement with B12 at recommended doses, don’t take more than you need, and don’t be alarmed by studies linking high blood B12 to disease.
Introduction
Vitamin B12 deficiency results in fatigue due to poorly formed red blood cells, and can cause neurological problems, including tingling in the fingers and toes, difficulty walking, and cognitive problems such as memory loss and confusion.
Because B12 isn’t naturally found in plants (A), vegans need to obtain it through fortified foods and supplements. Omnivores can obtain B12 from animal products, though absorption often decreases with age.
Neither the Institute of Medicine nor the European Food Safety Authority has set an upper limit for B12 intake (IOM, 1998; EFSA, 2015). Nevertheless, some observational evidence raises questions worth examining, which this page reviews.
For reference, sources for normal B12 levels vary: Mayo Clinic (2020) lists 133–677 pmol/l (180–914 pg/ml; 1 pmol/l = 1.36 pg/ml). Arendt et al. (2016) list 200–600 pmol/l (271–813 pg/mL). Plasma and serum vitamin B12 levels have been found to be essentially the same (Sviland, 1985).
Elevated B12 as a Marker for Disease: Serum B12 and Mortality
Elevated B12 levels have long been considered a marker, but not a cause, of numerous diseases. Except for some unusual findings for lung cancer discussed below, associations between elevated serum B12 and increased disease or mortality are most plausibly explained by reverse causation, in which underlying disease raises B12 levels rather than elevated B12 causing disease. The studies reviewed here generally support this interpretation, either finding no association after appropriate adjustment or failing to adjust for kidney and liver function at all. These studies don’t measure B12 intakes, so no correlations between intakes and serum levels can’t be determined.
Liver disease and cancer. The liver stores a large portion of the body’s B12, and many liver diseases can elevate serum B12. Researchers at the National Institutes of Health found, in intensive care unit patients, a strong correlation between elevated B12 levels and risk of death, but the correlation disappeared after adjusting for liver function (Callaghan, 2014). A French study found a strong association with elevated serum B12 and cirrhosis and hepatitis (Deneuville, 2009). Various cancers can also cause elevated serum B12, including cancers of the upper gastrointestinal tract, liver, pancreas, lungs, and bone marrow; elevated B12 in these cases is indicative of undiagnosed cancer rather than a cause of it (Arendt, 2016; Arendt, 2019; Andres, 2013).
Kidney disease. Moderately impaired kidney function can cause elevated B12 levels. The Framingham Heart Study found that elevated B12 at baseline was associated with two markers of impaired kidney function, but, upon follow-up, a previously elevated B12 was not associated with a future diagnosis of either condition — meaning poor kidney function most likely caused the elevated B12, not vice versa (McMahon, 2015).
Prevention of Renal and Vascular End-stage Disease (PREVEND), a prospective cohort study from the Netherlands, oversampled for people with poor kidney function and found that plasma B12 >337 pmol/l was associated with an 85% increased risk of early death (HR 1.85, CI 1.16–2.97) after an average of 8.2 years of follow-up (Flores-Guerrero, 2020). When excluding those with mildly to moderately impaired kidney function, the remaining findings would not survive false discovery rate correction in the fully adjusted models. Cancer and cardiovascular mortality were null throughout.
Prospective studies in older or semi-healthy populations. Among relatively healthy populations at baseline, prospective studies in people over 60 have produced mixed results, with some finding associations between elevated B12 and mortality (Mendonca, 2018; Gonzalez, 2007; Zeitlin, 1997; Xu, 2021) and others finding none (Dangour, 2008; Jia, 2007; Hung, 2003). Studies that found associations generally didn’t adjust for kidney or liver function.
Studies in sick populations. At least eleven studies have measured the relationship between elevated B12 and mortality or morbidity in populations known or suspected to have an illness, typically to determine if elevated B12 is an indicator of particular diseases (Arendt, 2013; Arendt, 2016; Arendt, 2019; Callaghan, 2014; Hemmersbach-Miller, 2005; Huang, 2012; Robinson, 2011; Ryg, 2013; Salles, 2005; Sviri, 2012; Valdivia, 2020). These studies are not designed to determine whether excess B12 intake is unhealthy.
Macro-B12
Elevated serum B12 can sometimes be due to a phenomenon called macro-B12, in which B12 forms complexes with immunoglobulins that accumulate in the blood due to reduced clearance. These complexes are biologically inactive, and no harm from them has been detected. Standard B12 blood tests strip B12 off all its carrier proteins and measure the total freed B12, so they can’t distinguish between normal B12 and macro-B12: both contribute equally to the reading. A 2024 critical review noted that unexpectedly high B12 levels can be further investigated by a clinician if needed, preferably by directly measuring the carrier proteins haptocorrin and transcobalamin rather than relying on the commonly ordered PEG precipitation test, which the authors found nonspecific and potentially misleading (Fedosov, 2024). Vegans with unexplained elevated serum B12 who are not taking high-dose supplements may want to mention this possibility to their doctor.
B12 Supplementation Trials
The ideal way to examine the dangers of B12 supplementation would be to design a study whose primary purpose is to assess this possibility, before choosing a population and taking measurements. Unfortunately, there are no studies like this. However, many clinical trials have examined whether lowering homocysteine levels through folic acid, vitamin B12, and vitamin B6 supplementation can reduce cardiovascular disease events, typically in people with a history of cardiovascular disease; some of these studies have monitored side effects.
For a detailed review of these trials and their cancer-related findings, see Table 2. B-Vitamin RCTs: All-cause Mortality and Secondary Cancer Outcomes on the Folic Acid page. Most trials found no significant association between B-vitamin supplementation and cancer. The most concerning findings come from two trials using folic acid combined with 400–500 µg/day of B12:
- Ebbing (2009) found a statistically significant increase in overall cancer incidence (RR 1.21, CI 1.03–1.41)
- B-PROOF found an increased risk of colon cancer (HR 2.17, CI 1.26–3.75) in the per-protocol analysis (Oliai Araghi, 2019).
Given that the populations were typically unhealthy, this isn’t enough to drive B12 recommendations, but it suggests that avoiding excess amounts is prudent.
B12 Observational Studies
Table 1 below summarizes the observational studies most relevant to supplement B12 safety in healthy adults. Unlike the serum B12 studies above, these studies either measured supplement doses directly (Wolffenbuttel, 2020; Brasky, 2017) or used pre-diagnostic circulating B12 in prospective cohorts with sufficient lead time to reduce reverse causation concerns (Fanidi, 2019).
The only large study of healthy adults examining B12 supplement safety, using NHANES data, found no association between B12 supplementation and increased mortality at any dose, including 1,000 µg/day or more (Wolffenbuttel, 2020). The VITAL cohort (Brasky, 2017) found a near-doubling of lung cancer risk in men taking >55 µg/day of B12 from individual supplements, but the dose-response trend across all men was not statistically significant (p-trend=0.12), and the significant trend appeared only in the current-smoker subgroup, a pre-specified but secondary analysis in a small subgroup with no multiplicity correction applied. The Fanidi (2019) findings are discussed in the following section.
Vitamin B12 and Lung Cancer
The LC3 Nested Case-Control Study
A 2019 nested case-control study compiled pre-diagnostic blood samples from 5,183 lung cancer case-control pairs drawn from 20 prospective cohorts (Fanidi, 2019). Participants with B12 levels of 426–531 pmol/l (OR 1.16, CI 1.03–1.30) and >531 pmol/l (OR 1.19, CI 1.05–1.34) had an overall lung cancer odds ratio of 1.15 (1.06–1.25) per doubling of circulating B12 (p-trend=0.0009). Results were consistent across sexes, smoking strata, and geographic regions. The results weren’t adjusted for kidney function, which would normally lead me to dismiss them, given that smoking can damage kidney function over time, raising B12 levels independently of any causal relationship with lung cancer. However, the study matched for smoking status in five categories and additionally adjusted for cotinine, which should have substantially reduced confounding from smoking-related kidney damage. The study didn’t adjust for liver function, though adjusting for alcohol consumption didn’t change the results.
To put this finding in practical terms: If 2,000 people shifted their circulating B12 from the lowest quartile (<338 pmol/L) to the highest (>531 pmol/L), one additional lung cancer case would be expected over approximately 6 years. Both levels are within the normal range, and the absolute increase in risk per individual is small.
The Mendelian Randomization
To test whether the LC3 finding reflects a causal relationship rather than reverse causation, Fanidi et al. (2019) also conducted an independent Mendelian randomization (MR) analysis using an entirely separate population of 29,266 lung cancer cases and 56,450 controls from the TRICL-ILCCO consortium. Rather than measuring B12 directly, the MR used 8 genetic variants (SNPs) known to raise B12 levels as a proxy for lifelong B12 levels. Because these genetic variants are fixed at conception and cannot be altered by disease, they sidestep the reverse causation problem that affects observational studies.
The MR finding was OR 1.08 (1.00–1.16) per 150 pmol/L increase in genetically predicted B12 for overall lung cancer, with the strongest signal for adenocarcinoma (OR 1.23, 1.11–1.37), the most common subtype to be diagnosed in people who have never smoked (Patel, 2026). The 8 SNPs showed no association with smoking behavior in an independent dataset of 74,035 participants, ruling out smoking as a confounding pathway through the genetic instrument. The MR finding is stronger causal evidence than the LC3 observational findings in the previous section, because genetically predicted B12 cannot be influenced by disease or reverse causation. But its precision is limited by a borderline lower confidence interval (1.00) and by the fact that the 8 SNPs explain only 5.1% of the variance in B12.
VITAL
The Vitamins and Lifestyle Cohort found an increase in lung cancer among male smokers in the highest B12 intake group of 55–275 µg/day (Brasky, 2017). However, Obeid and Pietrzik (2018) argued this likely reflects reverse causality from health-anxious smokers selectively taking supplements.
At this time, the evidence is suggestive but not conclusive that high circulating B12 may modestly increase lung cancer risk. There isn’t enough evidence to warrant separate B12 recommendations for vegans, but it’s a reason to avoid unnecessarily high supplement doses.
| Table 1. Vitamin B12 Observational Studies | |||
|---|---|---|---|
| Study | Design / Exposure | Findings | Limitations |
| Wolffenbuttel, 2020 NHANES United States |
Prospective cohort n=24,262 (mean age 48 ± 19 yrs) NHANES surveys 1999–2014 linked to National Death Index Median follow-up 109 months (~9 yrs) 3,023 deaths (12.5%) Exposures assessed at baseline: • Daily oral B12 supplement: none, 0.1–4.9, 5–24.9, 25–99, 100–999, ≥1,000 µg/d • sB12: <140, 140–300, 300–700, >700 pmol/L |
Supplement B12 intake: No association with all-cause, cardiovascular, or cancer mortality at any dose category, including ≥1,000 µg/d sB12 reference group: 300–700 pmol/L |
Supplement intake self-reported; no repeated measurements. Cancer incidence NR, only cancer mortality. |
| Brasky, 2017 VITAL United States Western WA |
Prospective cohort Women=40,069, men=37,049 Ages 50–76 at enrollment 808 incident invasive lung cancers 10-yr average daily dose of supplemental B12, B6, and folate, reported retrospectively at enrollment Mean follow-up 6 yrs via registry linkage |
Lung cancer: Male B12 >55 µg/d vs. none: 1.98 (1.32–2.97) p-trend 0.12 Male use of B12 from multivitamins only: null Female, all B12 doses and sources: null Pre-specified subgroups: Folate: null in both sexes at all doses |
All-cause mortality not ascertained. No multiplicity correction. P-trends weren’t significant for primary findings for men (Table 2). Significant p-trends only in current-smoker subgroup where n is small. Reverse causation might not be fully addressed by 1-yr lag analysis, but if health-anxious smokers were driving the association, you’d expect them to take multivitamins too. |
| Fanidi, 2019 LC3 North America, Europe, Asia, Australia |
Nested case-control of 20 prospective cohorts of >2,000,000 pp 5,183 case-control pairs Ages 44–72 at enrollment Median 6.4 yrs between blood draw and diagnosis Matched on age, sex, cohort, smoking status; adjusted for cotinine and education |
Lung cancer: Overall, per doubling of serum B12 (↑) 1.15 (1.06–1.25) p-trend 0.0009 Consistent across sexes, smoking strata, time from blood draw, and geographic regions Adenocarcinoma 1.14 (1.00–1.30) NNH: ~2,000 people shifting from Q1 (<338 pmol/L) to Q4 (>531 pmol/L) for one additional lung cancer case over ~6.4 yrs. Estimated from: Q1 baseline risk ~0.26% over 6 years (5,183 cases / 2,000,000 cohort over 6.4 yrs), Q4 adjusted OR 1.19, absolute risk difference ~0.049%. |
No adjustment for kidney function or liver function. Alcohol adjustment didn’t change results. Both Q1 and Q4 are within the normal B12 range. |
| Fanidi, 2019 TRICL-ILCCO European descent Supersedes: Johansson, 2010 |
Genetic case-control, Mendelian randomization 29,266 lung cancer cases and 56,450 controls with no lung cancer, drawn from TRICL-ILCCO (entirely different participants than LC3). No follow-up period; a single snapshot comparison of genotype between those with and without lung cancer. B12 not directly measured: 8 SNPs associated with higher B12 used as proxy. |
Lung cancer per 150 pmol/L increase in genetically predicted B12: (↑) 1.08 (1.00–1.16)
Adenocarcinoma: 1.23 (1.11–1.37) MR-Egger pleiotropy test: p=0.17 (null) |
SNPs explain 5.1% of B12 variance. Two SNPs are associated with homocysteine and autoimmune disease, so potential pleiotropy not fully excluded. |
|
✗Nominally significant but likely does not survive Benjamini-Hochberg false discovery rate correction given the number of comparisons in this study. aFrom private correspondence with author. Abbreviations
|
|||
Cyanocobalamin, Cyanide, and Kidney Disease
There are four forms of vitamin B12, differentiated by the side group attached to the cobalamin molecule: adenosylcobalamin, cyanocobalamin, hydroxocobalamin, and methylcobalamin. Cyanocobalamin is the form most commonly found in supplements and fortified foods. Although methylcobalamin and adenosylcobalamin are the two coenzyme forms required for the body’s chemical reactions, their supplementation isn’t more efficient than cyanocobalamin or hydroxocobalamin because all B12 forms must first be stripped of their side groups before conversion to the coenzyme forms (Obeid, 2015).
A reasonable person might wonder why a chemical as dangerous as cyanide would be part of a nutritional supplement. Cobalamin has an especially strong affinity for cyanide, making cyanocobalamin a highly stable form of B12 and therefore suitable for fortified foods and supplements. In fact, one of the main ways to treat cyanide toxicity is through injections of hydroxocobalamin, as the cobalamin will lose the hydroxyl side group, pick up the cyanide, and then be excreted in the urine (FDA, 2018).
Cyanide is also found in foods as sugar-cyanide complexes known as cyanoglycosides and is ingested in small amounts on a regular basis (EFSA, 2019). Cyanoglycosides are found in at least 2,000 plants (WHO, 2004) and in many foods such as baked goods, stone fruits and their juices, almonds, legumes, and grains. The cyanide can become detached from the sugar after ingestion and must be detoxified, usually by the enzyme rhodanese, which converts cyanide to thiocyanate, which is then excreted in the urine.
For a 140 lb (63.5 kg) person, the average daily cyanide intake from food and air is 113 to 164 µg per day. A 1,000 µg dose of cyanocobalamin provides an additional 19.2 µg of cyanide (B), increasing daily intake by 12% to 20%. However, it only increases the percentage of the EFSA’s acute reference dose (ARfD) of 20 µg/kg body weight from 7.4% to 8.9% (lower bound) or from 13% to 15% (upper bound), which is negligible for people with normal kidney function.
The graph below compares those amounts to the ARfD.
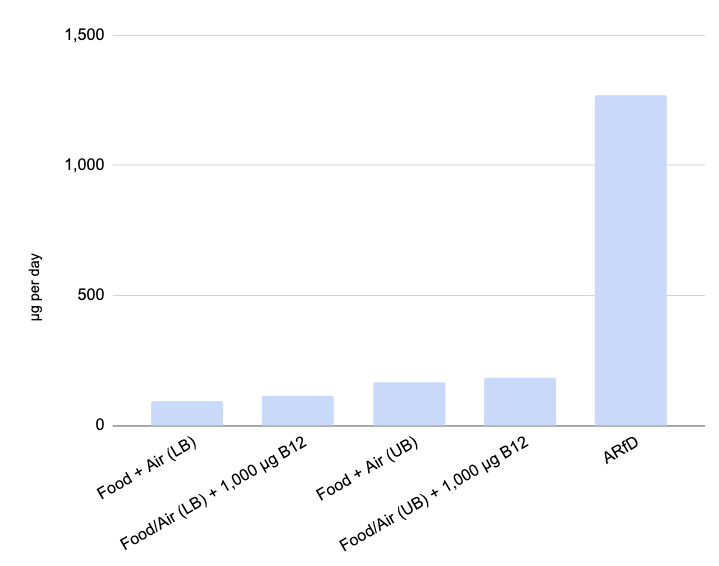
Note: The EFSA data for cyanide intake uses a lower bound and upper bound method to account for cyanide amounts below the detection or quantification levels (EFSA, 2019, p. 16).
Tobacco smoke also contains cyanide, 10 to 400 µg per cigarette for direct smoking (ATSDR, 2006). The Institute of Medicine reports mixed results on whether smokers excrete more B12 than nonsmokers, but concludes that the effect of smoking on B12 requirements appears to be negligible (IOM, 1998).
Thiocyanate, a byproduct of cyanide detoxification, can also harm the thyroid gland by competing with iodine, though this is generally observed only in populations exposed to high levels of cyanide through occupational sources or diets extremely high in cyanoglycosides, typically in regions with low soil iodine (Amar, 2015).
Kidney disease: Due to the cyanide in cyanocobalamin, we recommend that people with impaired kidney function avoid cyanocobalamin supplements. The strongest evidence comes from the DIVINe clinical trial, in which people with diabetic nephropathy taking 1,000 µg/day of cyanocobalamin (plus folic acid and B6) experienced significantly faster decline in kidney function than the placebo group over 36 months (5.8 mL/min/1.73 m² greater decline, p=0.02; House, 2010). By contrast, a shorter 12-week study in children with early-stage diabetic nephropathy found that the same dose improved kidney function (Elbarbary, 2020), suggesting that harm may be more likely in advanced kidney disease. Until more is known, high-dose cyanocobalamin should generally not be recommended for people with kidney disease.
Practical Implications
VeganHealth’s B12 recommendations are designed to meet two different targets: the lower end meets the Institute of Medicine’s recommended dietary allowance (RDA) of 2.4 µg/day, and the higher end meets the European Food Safety Authority’s adequate intake (AI) of 4.0 µg/day (see Rationale for VeganHealth’s B12 Recommendations; note that these absorption rates are for cyanocobalamin). The EFSA set its AI based on biomarker data showing no additional benefit above that level, and noted that it aligns with typical European dietary intakes of 4.2–8.6 µg/day. Using Walsh’s absorption formula (described here), the EFSA’s AI works out to a target absorption of 14.9 µg per week from food.
For context, the VITAL cohort found elevated lung cancer risk in men averaging ~127 µg/day from individual B12 supplements. The median dietary B12 intake across the VITAL cohort was 6.42 µg/day, resulting in ~19.1 µg of B12 absorbed per week from food. Adding the ~16.2 µg absorbed per week from the average of 127 µg/day of supplemental B12 for those in the high-risk Brasky group, gives a total of roughly 35.3 µg absorbed per week. VeganHealth’s higher-end recommendations result in less than half the total amount absorbed compared to the high-risk Brasky group; for example, a weekly B12 dose of 2,500 µg yields approximately 14.2 µg of absorption.
This doesn’t eliminate concern entirely, since we don’t know exactly how absorbed amounts translate into serum levels, and the Fanidi LC3 study found associations with lung cancer at serum B12 levels >531 pmol/L, which some vegans seem to achieve even at moderate supplement doses. But it does suggest that vegans following VeganHealth’s recommendations are absorbing considerably less B12 than those associated with elevated risk in the observational literature.
Regarding the lung cancer findings: With a number needed to harm of approximately 2,000 over six years, the absolute risk increase for any individual is small. The evidence comes from people with a greater amount of B12 absorbed than vegans supplementing at VeganHealth’s recommended doses, so sticking to our recommendations is prudent.
If your serum B12 is unexpectedly high despite supplementing at recommended doses, the first step is to investigate rather than immediately reduce your supplemental dose. As discussed above, elevated serum B12 is often a marker of underlying conditions rather than a direct consequence of supplementation. Reducing B12 supplementation without understanding why B12 is elevated risks creating a B12 deficiency that is a far more established health problem than the modest lung cancer signal this article describes. First, confirm you’re not supplementing above the recommended amounts. If you’re not, consider talking to your healthcare provider about:
- Ruling out macro-B12 (biologically inactive B12-immunoglobulin complexes that inflate the total B12 reading).
- Checking kidney and liver function, both of which can raise circulating B12 when impaired.
Some people might suggest that the lung cancer findings discussed above could be explained by the cyanide in cyanocobalamin rather than by B12 itself. This is unlikely for two reasons. First, a 1,000 µg dose of cyanocobalamin provides only 19.2 µg of cyanide, a trivial addition to the 113 to 164 µg already ingested daily from food and air. Second, and more importantly, the two strongest studies linking B12 status to lung cancer, the Fanidi LC3 nested case-control and the Mendelian randomization, measured circulating B12 in populations getting B12 primarily from food, where the predominant forms aren’t cyanocobalamin. The association, therefore, appears to involve B12 itself rather than the cyanide moiety.
B12 Supplements and Skin Rashes
Summary. Rare cases of people developing or exacerbating skin rashes from vitamin B12 injections have been documented. Even rarer are people who develop rashes from oral B12 supplementation. People with acne who take high-dose oral vitamin B12 should be aware that, while rare, it could possibly trigger a breakout. People with known cobalt sensitivities should be aware that vitamin B12 contains cobalt.
Why B12 might trigger rashes. Kang et al. (2015, UCLA) conducted a small study providing a plausible biological explanation for why B12 supplementation may trigger acne in some individuals. P. acnes lives in the hair follicle (as distinct from the gut), and elevated serum B12 reaches it through the bloodstream. Kang et al. cite Stankler (1969) in noting that skin B12 levels correlate with serum B12 levels. The researchers found that elevated B12 suppresses P. acnes‘s own B12 biosynthesis pathway, redirecting metabolic precursors toward porphyrins, which induce skin inflammation. A follow-up in vitro study by the same group found this response is strain-specific, with acne-associated P. acnes strains producing more porphyrins in response to B12 while health-associated strains did not (Johnson, 2016, UCLA).
Clinical evidence. Most of the clinical evidence involves injections rather than oral supplements. Kang et al. monitored ten subjects receiving 1,000 µg hydroxocobalamin injections; one developed acne within a week. A single injection can raise serum B12 to between 1,500 and 57,000 pg/mL for at least two weeks, far above levels typically seen with oral supplementation. A case series reported five women who developed acneiform eruptions from B12 therapy: three from injections alone, one from combined B12 and B6 injections, and one from an oral B-vitamin combination; all had complete spontaneous remission within three to six weeks of discontinuation (Veraldi, 2018). Another case report described rosacea fulminans two weeks after a teenager began a B-complex supplement containing 20 µg of B12 and 80 mg of B6; the authors attributed this primarily to the B6 dose, making it of limited relevance to B12 supplementation (Jansen, 2001). Sanz-Cuesta (2020) found that among 283 patients, 3 of 143 receiving injections developed a rash compared to 2 of 140 taking 1,000 µg/day orally, a small difference consistent with the mechanistic picture.
Cobalt allergies. People with a known cobalt allergy, typically identified by reactions to metal jewelry or implants, may occasionally react to vitamin B12 supplements because cobalt is a structural component of all cobalamins. Reactions, where they occur, tend to involve the skin: contact dermatitis, hives, or, in rare cases, hyperpigmentation. Though the evidence base is limited to a small number of case reports, those with known cobalt allergy are advised to discuss B12 supplementation with a clinician before starting (MHRA, 2023).
Desensitization protocols. Lis (2025) describes desensitization protocols for patients who have developed sensitivity to B12 injections. The underlying evidence consists of a handful of case reports, but it might be helpful for clinicians.
Practical implications. Since it’s absorbed B12, not the supplemental dose, that reaches skin bacteria, and since oral supplementation produces far lower serum levels than injectable B12, the risk of acne from oral supplementation is considerably lower than from injections. We’re not aware of research on whether the modest serum elevations from oral supplementation have similar effects on skin bacteria. Those who notice new or worsening acne after beginning B12 supplementation may find it worth trying lower doses.
Footnotes
A. When vitamin B12 is injected into the soil around a plants’ roots, some plants can absorb a portion of it, but this isn’t a practical source of B12 in the food supply. Various algae have been shown to contain vitamin B12 and its analogs, but no algae in practical amounts have been found to improve B12 status in humans. For more information, see B12 in Plant Foods.
B. In determining what a safe level of cyanocobalamin might be, it would be helpful to know how much cyanide in a dose of cyanocobalamin is absorbed into the system. The cyanide that isn’t absorbed would be excreted in the feces, preventing harm to the kidneys.
Molecular weight of cyanide = 26.02 g/mol
Percentage of cyanocobalamin as cyanide = 1.92%
Cyanide in 1,000 µg dose of cyanocobalamin = 19.2 µg
A 2010 study found that a major fraction of cyanocobalamin stays intact during the process of being absorbed and delivered to the cells (Hardlei, 2010). To be safe, we’ll assume that all cyanide from a dose of cyanocobalamin is liberated, absorbed, and that the body must detoxify it, via the kidneys.
Bibliography
Amar K, C. Iodine, Thiocyanate and the Thyroid. Biochemistry & Pharmacology: Open Access, 04(03). 2015.
Andrès E, Serraj K, Zhu J, Vermorken AJ. The pathophysiology of elevated vitamin B12 in clinical practice. QJM. 2013;106:505–515.
Arendt JF, Pedersen L, Nexo E, Sørensen HT. Elevated plasma vitamin B12 levels as a marker for cancer: a population-based cohort study. J Natl Cancer Inst. 2013;105:1799–1805.
Arendt JF, Farkas DK, Pedersen L, Nexo E, Sørensen HT. Elevated plasma vitamin B12 levels and cancer prognosis: a population-based cohort study. Cancer Epidemiol. 2016;40:158–165.
Arendt JFH, Sørensen HT, Horsfall LJ, Petersen I. Elevated Vitamin B12 Levels and Cancer Risk in UK Primary Care: A THIN Database Cohort Study. Cancer Epidemiol Biomarkers Prev. 2019;28(4):814–821.
Armitage JM, Bowman L, Clarke RJ, Wallendszus K, Bulbulia R, Study of the Effectiveness of Additional Reductions in Cholesterol and Homocysteine (SEARCH) Collaborative Group. Effects of homocysteine-lowering with folic acid plus vitamin B12 vs placebo on mortality and major morbidity in myocardial infarction survivors: a randomized trial. JAMA. 2010;303:2486–94.
Agency for Toxic Substances and Disease Registry. Toxicological Profile For Cyanide. U.S. Department Of Health And Human Services. Public Health Service. July 2006.
Brasky TM, White E, Chen CL. Long-Term, Supplemental, One-Carbon Metabolism-Related Vitamin B Use in Relation to Lung Cancer Risk in the Vitamins and Lifestyle (VITAL) Cohort. J Clin Oncol. 2017 Aug 22:JCO2017727735. Note: The 127 µg male smoker average comes from private correspondence (see table note).
Callaghan FM, Leishear K, Abhyankar S, Demner-Fushman D, McDonald CJ. High vitamin B12 levels are not associated with increased mortality risk for ICU patients after adjusting for liver function: a cohort study. ESPEN J. 2014 Apr 1;9(2):e76-e83.
Dangour AD, Breeze E, Clarke R, Shetty PS, Uauy R, Fletcher AE. Plasma homocysteine, but not folate or vitamin B-12, predicts mortality in older people in the United Kingdom. J Nutr. 2008;138(6):1121–1128.
Deneuville T, Mario N, Tiev KP, Tolédano C, Josselin-Mahr L, Gain M, et al. Concentration plasmatique élevée de la vitamine B12: un indicateur des maladies hépatiques ou tumorales? Rev Med Interne. 2009;30(Suppl. 2):S73.
Ebbing M, Bønaa KH, Nygård O, Arnesen E, Ueland PM, Nordrehaug JE, Rasmussen K, Njølstad I, Refsum H, Nilsen DW, Tverdal A, Meyer K, Vollset SE. Cancer incidence and mortality after treatment with folic acid and vitamin B12. JAMA. 2009 Nov 18;302(19):2119-26.
European Food Safety Authority NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies), 2015. Scientific Opinion on Dietary Reference Values for cobalamin (vitamin B12). EFSA Journal 2015;13(7):4150, 64 pp.
European Food Safety Authority Panel on Contaminants in the Food Chain. Scientific opinion on the evaluation of the health risks related to the presence of cyanogenic glycosides in foods other than raw apricot kernels. EFSA Journal. 2019;17(4):5662, 78 pp.
Elbarbary NS, Ismail EAR, Zaki MA, Darwish YW, Ibrahim MZ, El-Hamamsy M. Vitamin B complex supplementation as a homocysteine-lowering therapy for early stage diabetic nephropathy in pediatric patients with type 1 diabetes: A randomized controlled trial. Clin Nutr. 2020 Jan;39(1):49-56.
Fanidi A, Muller DC, Yuan JM, et al. Circulating Folate, Vitamin B6, and Methionine in Relation to Lung Cancer Risk in the Lung Cancer Cohort Consortium (LC3). J Natl Cancer Inst. 2018 Jan 1;110(1):57–67.
Fanidi A, Carreras-Torres R, Larose TL, et al. Is high vitamin B12 status a cause of lung cancer? Int J Cancer. 2019;145(6):1499-1503.
U.S. Food and Drug Administration. CYANOKIT® (hydroxocobalamin for injection) for intravenous infusion. Initial U.S. Approval: 1975. Revised: 12/2018. Reference ID: 4369589.
Fedosov SN, Nexo E. Macro-B12 and Unexpectedly High Levels of Plasma B12: A Critical Review. Nutrients. 2024 Feb 26;16(5):648.
Flores-Guerrero JL, Minovic I, Groothof D, Gruppen EG, Riphagen IJ, Kootstra-Ros J, Muller Kobold A, Hak E, Navis G, Gansevoort RT, de Borst MH, Dullaart RPF, Bakker SJL. Association of Plasma Concentration of Vitamin B12 With All-Cause Mortality in the General Population in the Netherlands. JAMA Netw Open. 2020 Jan 3;3(1):e1919274.
González S, Huerta JM, Fernández S, Patterson AM, Lasheras C. Homocysteine increases the risk of mortality in elderly individuals. Br J Nutr. 2007 Jun;97(6):1138-43.
Hardlei TF, Mørkbak AL, Bor MV, Bailey LB, Hvas AM, Nexo E. Assessment of vitamin B(12) absorption based on the accumulation of orally administered cyanocobalamin on transcobalamin. Clin Chem. 2010 Mar;56(3):432-6.
Hemmersbach-Miller M, Conde-Martel A, Betancor-León P. Vitamin B as a predictor of mortality in elderly patients. J Am Geriatr Soc. 2005;53(11):2035–2036.
House AA, Eliasziw M, Cattran DC, Churchill DN, Oliver MJ, Fine A, Dresser GK, Spence JD. Effect of B-vitamin therapy on progression of diabetic nephropathy: a randomized controlled trial. JAMA. 2010 Apr 28;303(16):1603-9.
Huang YC, Lee MS, Wahlqvist ML. Prediction of all-cause mortality by B group vitamin status in the elderly. Clin Nutr. 2012;31(2):191–198.
Hung J, Beilby JP, Knuiman MW, Divitini M. Folate and vitamin B-12 and risk of fatal cardiovascular disease: cohort study from Busselton, Western Australia. BMJ. 2003;326(7381):131.
Institute of Medicine. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline. Washington, DC: The National Academies Press; 1998.
Jansen T, Romiti R, Kreuter A, Altmeyer P. Rosacea fulminans triggered by high-dose vitamins B6 and B12. J Eur Acad Dermatol Venereol. 2001 Sep;15(5):484-5.
Jia X, Aucott LS, McNeill G. Nutritional status and subsequent all-cause mortality in men and women aged 75 years or over living in the community. Br J Nutr. 2007;98(3):593–599.
Johansson M, Relton C, Ueland PM, et al. Serum B vitamin levels and risk of lung cancer. JAMA. 2010 Jun 16;303(23):2377-85. Superseded by Fanidi, 2019.
Johnson T, Kang D, Barnard E, Li H. Strain-Level Differences in Porphyrin Production and Regulation in Propionibacterium acnes Elucidate Disease Associations. mSphere. 2016 Feb 10;1(1):e00023-15.
Kang D, Shi B, Erfe MC, Craft N, Li H. Vitamin B12 modulates the transcriptome of the skin microbiota in acne pathogenesis. Sci Transl Med. 2015 Jun 24;7(293):293ra103.
Lis K. Desensitization for Vitamin B12 Hypersensitivity and How to Do It. Biomedicines. 2025 Mar 26;13(4):801.
Test Definition: B12. Vitamin B12 Assay, S. Mayo Clinic Laboratories. Accessed August 7, 2020.
McMahon GM, Hwang SJ, Tanner RM, Jacques PF, Selhub J, Muntner P, Fox CS. The association between vitamin B12, albuminuria and reduced kidney function: an observational cohort study. BMC Nephrol. 2015 Feb 2;16:7.
Mendonça N, Jagger C, Granic A, Martin-Ruiz C, Mathers JC, Seal CJ, Hill TR. Elevated Total Homocysteine in All Participants and Plasma Vitamin B12 Concentrations in Women Are Associated With All-Cause and Cardiovascular Mortality in the Very Old: The Newcastle 85+ Study. J Gerontol A Biol Sci Med Sci. 2018 Aug 10;73(9):1258-1264.
Medicines and Healthcare products Regulatory Agency. United Kingdom. Vitamin B12 (hydroxocobalamin, cyanocobalamin): advise patients with known cobalt allergy to be vigilant for sensitivity reactions. Drug Safety Update volume 17, issue 5: December 2023: 2.
National Institutes of Health. Office of Dietary Supplements (ODS). Vitamin B12 Fact Sheet for Health Professionals. Updated March 30, 2020. Accessed June 3, 2020.
Obeid R, Fedosov SN, Nexo E. Cobalamin coenzyme forms are not likely to be superior to cyano- and hydroxyl-cobalamin in prevention or treatment of cobalamin deficiency. Mol Nutr Food Res. 2015 Jul;59(7):1364-72.
Obeid R, Pietrzik K. Smoking, B Vitamins, and Lung Cancer: The Chicken or the Egg Causality Dilemma. J Clin Oncol. 2018;36(6):626-627.
Oliai Araghi S, Kiefte-de Jong JC, van Dijk SC, Swart KMA, van Laarhoven HW, van Schoor NM, de Groot LCPGM, Lemmens V, Stricker BH, Uitterlinden AG, van der Velde N. Folic Acid and Vitamin B12 Supplementation and the Risk of Cancer: Long-term Follow-up of the B Vitamins for the Prevention of Osteoporotic Fractures (B-PROOF) Trial. Cancer Epidemiol Biomarkers Prev. 2019 Feb;28(2):275-282.
Patel A, Bhimani N, Bhimani C. Lung Adenocarcinoma. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026.
Robinson DJ, O’Luanaigh C, Tehee E, et al. Vitamin B12 status, homocysteine and mortality amongst community-dwelling Irish elders. Ir J Med Sci. 2011;180(2):451–455.
Ryg J, Nybo M, Hallas J. Cancer incidence in persons with elevated cobalamin levels. Eur J Clin Invest. 2013;43(6):557–561.
Salles N, Herrmann F, Sakbani K, Rapin CH, Sieber C. High vitamin B12 level: a strong predictor of mortality in elderly inpatients. J Am Geriatr Soc. 2005;53:917–8.
Sanz-Cuesta T, Escortell-Mayor E, Cura-Gonzalez I, et al. Oral versus intramuscular administration of vitamin B12 for vitamin B12 deficiency in primary care: a pragmatic, randomised, non-inferiority clinical trial (OB12). BMJ Open. 2020;10(8):e033687.
Spence JD, Yi Q, Hankey GJ. B vitamins in stroke prevention: time to reconsider. Lancet Neurol. 2017 Sep;16(9):750-760.
Sviland L, Rodger RS, Fail JB, Hamilton PJ. EDTA plasma rather than serum for B12, folate and ferritin estimations? J Clin Pathol. 1985;38(10):1197.
Sviri S, Khalaila R, Daher S, et al. Increased Vitamin B12 levels are associated with mortality in critically ill medical patients. Clin Nutr. 2012;31(1):53-59.
Valdivia G, Navarrete C, Oñate A, et al. Asociación entre niveles de vitamina B-12 y mortalidad en pacientes hospitalizados adultos mayores [Association between high vitamin B12 levels and one year mortality in older people admitted to the hospital]. Rev Med Chil. 2020;148(1):46-53. (Spanish)
Veraldi S, Benardon S, Diani M, Barbareschi M. Acneiform eruptions caused by vitamin B12: A report of five cases and review of the literature. J Cosmet Dermatol. 2018 Feb;17(1):112-115.
World Health Organization. Hydrogen Cyanide And Cyanides: Human Health Aspects. Concise International Chemical Assessment Document 61. Geneva, 2004.
Wolffenbuttel BHR, Heiner-Fokkema MR, Green R, Gans ROB. Relationship between serum B12 concentrations and mortality: experience in NHANES. BMC Med. 2020 Oct 9;18(1):307.
Xu K, Liu X, Liu J, Zhang Y, Ding X, Li L, Sun J. Association between serum vitamin B12 and risk of all-cause mortality in elderly adults: a prospective cohort study. BMC Geriatr. 2021 Sep 16;21(1):497.
Zeitlin A, Frishman WH, Chang CJ. The association of vitamin b 12 and folate blood levels with mortality and cardiovascular morbidity incidence in the old old: the Bronx aging study. Am J Ther. 1997;4(7-8):275–281.